Skip to main content
443.849.2000
Header Secondary Utility Nav Menu
Billing & Estimates
Careers
Maps & Directions
New Patient Appointment
In this section
Back
Main Menu
Find a Doctor
Departments & Services
MyChart
Giving
About GBMC
About Us
Accreditations, Mission, & Vision
CEO Blog
Greater Facts
Leadership at GBMC
Our History
Our Physician Titans
Billing & Estimates
Pay a Bill
Need an Estimate?
Hospital & Physician Charges
Billing & Financial Support
Surprise Medical Bills
Good Faith Estimate
Blogs & News
CEO Blog
Greater Living
Podcasts
Pressroom
Careers
GBMC Career Center
Benefits & Wellness
Diversity & Inclusion
Employee Orientation
Equal Employment Opportunity Policy
Human Resources
Volunteers
Clinical Education
Contact Us
For Physicians
Crimson
Employee/Physician Citrix Login
Endoscopy Posting
EpicCare Link
Epic Dictation (M*Modal)
Epic Training for Physicians
Epic Training for Block Scheduling
E-Prescribing License
Focused Professional Practice Evaluation
Institutional Review Board
Lab Test Directory
Medical Staff Bylaws
Ortho Viewer
Outlook Email Web Application
Physician Relations
Provider Personalization / Optimization
Surgical Posting
Maps & Directions
Nursing at GBMC
Our Community
Community Benefit
Community Health Needs Assessment
Government Relations
Health Screenings
Opioid Epidemic Educational Resources
Philanthropy
Red Cross Blood Drive
Volunteers at GBMC
Patients & Visitors
Billing & Financial Support
The Boutique
Change HealthCare Cyberattack
The Corner Shop (Gift Shop)
Dining at GBMC
Ethics Consultation
Hospital & Physician Charges
Maps & Directions
Medical Records
Parking on GBMC Campus
Patient & Family Advisory Council
Privacy Rights and Non-Discrimination
Room Service
Spiritual Support
Your Visit to GBMC
Quality & Patient Safety
Visitor Policies
Volunteers
Dismiss Modal
Close
Providers
Services
MyChart
Giving
search
show off canvas menu
Patient Stories
Women in prayer shawl ministries put care and prayer into their creations
They Helped Us Fulfill Our Dreams
My Weightloss Journey - 5 Episode Series with Erin Wilson
Compassionate, Loving and Concerned Care
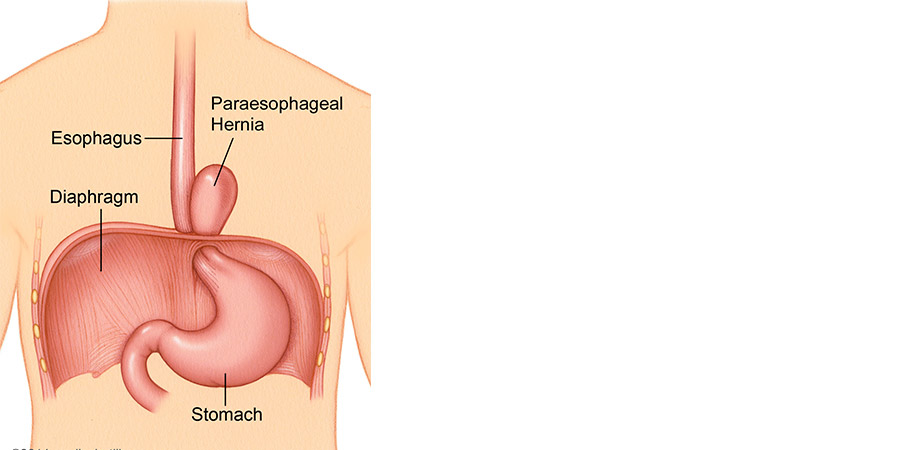
Rare Hernia is No Match for Skilled Surgeon
Weighing the Options: When is it time to consider weight loss surgery?
Into the Wilderness: Beyond Primary Care
Attorney Objects to Persistent Hoarseness
Care Management - A Healthy Dialogue with Ms. Watkins
Local Nurse Survives Cancer, Faces Non-healing Wound Decades Later
Preventive Procedure Helps Patient Rest Easy
Cause for Celebration: One Woman's Triumph over Breast Cancer
A Life Saved Twice: Gastric Bypass Patient Wins Colon Cancer Battle
Advancing Science With Clinical Trials
In Sickness and In Health
Pagination
First
Previous
...
4
5
6
7
8
9
10
11
12
Next
Last
The podcast that helps empower parents in the trenches
Learn More
Better Together | A Blog From GBMC's President and CEO
Learn More